
Intrauterine insemination (IUI) is a procedure commonly done in fertility clinics around the world. We place the sperm inside the uterus, close to the fallopian tubes, to increase the chances of conception.
If you’re going to do IUI treatment, you want it to work. Read along as I break down the steps to give you the best chance of success at IUI. I’ll take you through what I typically do with my patients to give you insight into what you can expect!
First things, first:
The TUSHY Method:

As you may know, my approach to fertility medicine is simple; understand your fertility diagnosis BEFORE treatment. There are five easy steps to figure to determine if IUI is the right treatment plan for you.
Tubes: We do a hysterosalpingogram (HSG) to make sure the fallopian tubes are open. This is an x-ray of the cavity of the uterus and fallopian tubes. If one tube is blocked and one tube is open you can still do IUI, but you want to make sure you’re monitoring which side you’re ovulating from.
Why? Your body does not evenly ovulate on each side. It’s literally a flip of the coin on which side you’ll ovulate on. Without monitoring with a pelvic ultrasound you would have no way of knowing which side you’re ovulating on and you don’t want to waste time on an IUI if you’re ovulating on the blocked side.
Uterus: An ultrasound of the uterus. I wish there was an easy way that people could look at their uterus without having to drive to my office, but we don’t have such a thing. Without a pelvic ultrasound, you wouldn’t know if you have cysts on your ovaries, a polyp inside your uterus, or a fibroid in the cavity that could block implantation. Get a pelvic ultrasound done before you consider IUI treatment.
Sperm: For obvious reasons you want to look at sperm health. There are so many things that you can do to get sperm to swim faster. Lifestyle factors and vitamins to name a couple. If there are sperm issues, make sure there’s isn’t a varicocele (enlargement of the veins in the scrotum), get your hormones checked and ask if there are any genetic tests that should be done first. Unless you check sperm health you wouldn’t know what you could do, on your own, to increase the chances of a healthy pregnancy without fertility treatment. It may sound funny coming from a fertility doctor, but I want you to get pregnant on your own! In a perfect world, nobody would need to see me!
Hormones: Cycle day 3 FSH, estradiol, AMH, TSH, and Prolactin. These are hormones that if not balanced can cause problems with fertility. Do a preconception blood panel to understand your levels and make sure you’re doing everything to treat any possible hormonal issues before IUI.
Your genetic profile: Make sure the egg and sperm are genetically compatible! I like to do preconception genetic testing before I start an IUI cycle.
Ultimately I want you to have the best chance of reaching the family size you desire. Plan for the future and ask if IUI at your age will help you reach your goals.
Ovulation
Let’s talk about the nuts and bolts of a fertility calendar.
Every month you only ovulate one egg, but some people have the potential to ovulate more than that. When you take fertility pills you typically may ovulate more than one.
Talk to your doctor about what the goal number of eggs is for your treatment and why, what the pregnancy rate is for IUI at your age with the drug regimen they have recommended, and how many cycles they expect to need to do for you to help you get to your pregnancy goals (and family size).
I tell my patients, “when your period starts, think of me.” I ask my patients to email me when their period starts on cycle day #1. Even if it’s a weekend. If your ovaries are working, so am I!
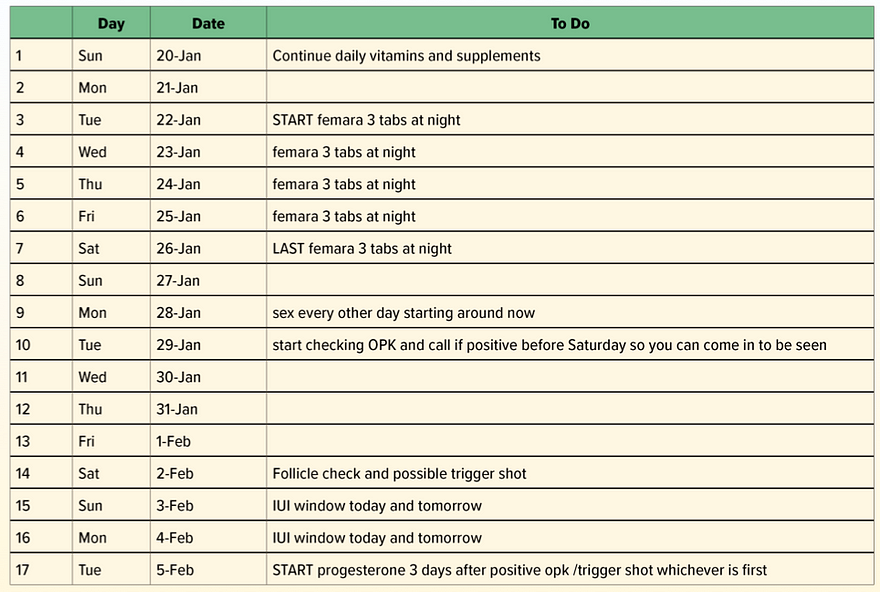
Once the period starts I look back at the “Personalized Fertility Care Plan” I have already summarized for them. I then create a calendar (example shown below) based on everything we have learned and review it with them. If a patient previously did treatment or has a history of cysts, I will have them come in for a pre-IUI cyst check, otherwise, I will review the calendar over the phone.
Let’s talk about Femara (aka letrozole). It has shown to have minor side effects in my patients such as mild headaches and slight nausea. That’s why I use it over Clomid because it’s better tolerated. However, there are things you can do to lessen these annoyances. Rather than taking 3 tablets, go down to 2. You may even consider taking 1 tablet—especially if you do not want a chance at twins. I tell my patients to take the medication at night so that they are sleeping when nausea may hit.
We start Femara on cycle day 3 as our body decides which egg it’s going to ovulate on day 5. Starting earlier gives you a higher chance that you can rescue an extra egg.
Yes, that’s right. I said rescue.
Fertility Doctors are really egg rescuers—we’re just throwing out life vests to your eggs so that you can ovulate an extra one. We want two chances for the sperm to hit one egg in a single cycle. A little myth-busting for you: working with a fertility doctor will not trigger the early onset of menopause nor reduce your overall number of eggs.
Sex
It’s not a taboo topic for me with patients. I talk about sex all day, every day in my office. I give my patients prescriptions for sex. I recommend intercourse—don’t abstain for sex. Practice makes perfect. Guys are preparing for the big day. I don’t want a bunch of dead swimmers for IUI day. We want healthy sperm and that comes from frequent ejaculation.
Ask your doctor about the sperm wash process there (assuming you are not using frozen sperm). We allow men to do their collection at home if the drive is under an hour and they are able to keep the sperm warm. You may laugh, but the best way to keep it warm is in a shirt pocket or in your bosom. I don’t require the male partner to bring it in. I tell guys to “flow and go.” Or the female partner can grab the cup and go too. But being there for each other on IUI day can only help. Lastly, avoid using lubricants during the collection that can hurt sperm. And don’t worry about not having enough. The volume of semen you need for an IUI barely covers the bottom surface of a specimen cup.
OPK:
The strategy is to NOT miss ovulation. If your OPK is positive before the follicle check day then I have patients come in immediately and we decide on an IUI window. On the follicle check day, we are measuring the size of the follicles and examine the thickness and texture of the lining of the uterus. I’m determining when the IUI should be done. When should those eggs be in the fallopian tube and put the sperm at the top of the uterus for the magic to happen? Timing is important, but there’s definitely a range. Once I’ve determined it’s time to do IUI planning, then we talk about the trigger shot.
The trigger shot sounds aggressive. I wish we could change the name! This is a small injection in the skin of your tummy approximately 36 hours before IUI. I base the timing of the injection on the size of the follicles, the thickness of the lining, and sperm strength (I do offer patients with lower sperm counts a double IUI and do the first IUI about 18 hours after the trigger shot and the second IUI 36 hours later).
The HCG trigger shot can be in your system for up to 10 days. Since it contains pregnancy hormone (it mimics the ovulation hormone LH so we use it to induce ovulation) and an at home pregnancy test will be positive if you check too soon.
Ask your doctor: How many eggs do you think are mature and when is the best day and time for my IUI?
After the IUI, the other thing that we do is start progesterone. It’s a hormone that helps with implantation.
Progesterone can be tricky for those with mood disorders. If you have depression you may want to talk with your doctor about your dosage and mode of administration.
You can take it orally or place it with your finger at the top of your vagina. What I’ve found is that when you place a medication vaginally you have fewer progesterone side effects (drowsiness and dizziness). If you still feel crummy you can reduce the dosage.
Remember, progesterone is promoting gestation so it’s a very, very good hormone for increasing the likelihood of conception! Think of it as water to a marathon runner. More is usually better!
Tips for Medication:
GoodRX.com
This has been a great resource for my patients who want to save money on drugs that don’t have a generic version or for patients that don’t have insurance. It’s a coupon saving site that will help direct you to the right pharmacy for the best price. (And no, I’m not getting paid in coupons from GoodRX.com to say this). Play around with it and you will see what I mean.
The IUI Procedure:

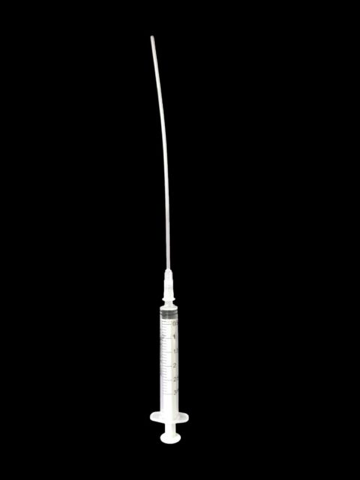
My goal is to place the speculum in the gentlest way possible. That said, for some patients who are very uncomfortable with a speculum, we may opt for one Valium 5 mg orally 30 minutes before (5% or less of patients need this) the procedure. I want you to be as comfortable as possible. I also ask my patients to come in with a full bladder (drink 3, 8-ounce glasses of water 2 hours before the appointment). Doing this allows the uterus to lean back and this makes the IUI catheter easier to place. I place a speculum and then place the catheter at the top of the uterus and shoot the swimmers in. I even give partners the chance to push the very end of the syringe to set the sperm free. It’s a special group moment.
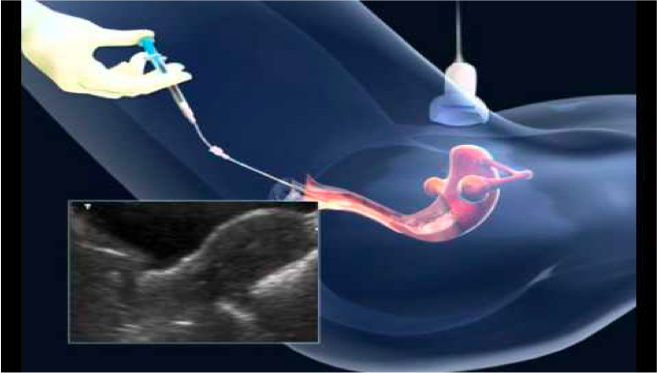
Sometimes I place an ultrasound over the lower abdomen to ensure the catheter is in the perfect place. If the catheter is hard to place at your next IUI, ask to wait for you to fill your bladder by drinking water and see if they have an ultrasound to help with better visualization.
In conclusion, I hope this was helpful to anyone considering IUI or currently in the process.
If you have a fertility question or there’s a topic you’d like me to cover in a future article or Egg Whisperer Show, please get in touch.
Send me a note: [email protected]
Catch more of me and topics like this through the Egg Whisperer Show. The episodes are live-streamed on YouTube, Facebook, and Twitter and on Wednesdays at 7 PM PST. Subscribe to the podcast too!
Thanks for this guide Dr Aimee! How do you ensure your patients have indeed ovulated? Thank you.
hi Kris! You’re welcome. The follicle check aka pelvic ultrasound is the most sensitive ovulation predictor kit. The trigger shot guarantees ovulation will happen and then what happens 2 weeks later also is a sign of ovulation: period or pregnancy. Always hoping for pregnancy. Here’s the thing though, I know that not all patients work with docs who do ultrasound monitoring or a trigger shot. Since all my patients are offered progesterone after ovulation, checking a progesterone level won’t be helpful. But the things patients can do to take things into their own hands would be to: get proovtest.com strips that can confirm ovulation and tell you if your progesterone level is normal. You can also do a blood draw for a progesterone level too. Great question!
HI Dr. Amiee
I had my trigger shot and iui done the same day. However, I have read the IUI normally happens 36 hours after trigger. Could the reason my RE did this be because I had a follicle that was 27cm x15cm?
Hi Dr Amy. After doing the trigger shot and IUI, how long does it take for the body to start making progesterone? I m having IUI. My dr prescribed to start progesterone 2 days IUI
I just did my first are you are a treatment but I did the trigger shot yesterday at 10 AM and they scheduled me to do my iui today at 11 .
I had three photos on one ovary and two of the other episodes of 20 so I don’t know I’ve been reading it says you should wait 36 hours to do are you why but it seems with this case scenario and was just the next day that set it after the trigger shot
Is this the same method used to implant an embryo into a surrogate mother? My husband and I have a surrogate mother to carry our child(ren) because I of my health.